
Werner D1524-2 Extension Ladder, 23 ft H Reach, 300 lb, ... - werner 48' extension ladder reach
B-Mode (Brightness Mode) in ultrasound is a setting that creates a two-dimensional (2D) greyscale image on your ultrasound screen and is the most commonly used mode. It is also commonly called 2D mode.
[…] knobs/buttons (depth, gain, focus, TGC, etc). In addition, the ultrasound will always start in B-mode or “greyscale” mode by […]
The good news is that all ultrasound machines have the same basic settings and once you understand them you can start using any ultrasound device with ease.
The most common POCUS applications for the endocavitary ultrasound probe are for intraoral (peritonsillar abscess) and transvaginal applications (early pregnancy, ovarian torsion, ovarian cyst, fibroids, ectopic pregnancy, etc). Make sure to always place a sterile endocavitary probe cover (condom or glove) prior to scanning.
Here is a video demonstrating all of these Pulse Wave Doppler steps to calculate the Velocity Time Integral of the left ventricular outflow tract:
I would suggest approaching any ultrasound machine in with the following order using the step-by-step approach below. I’ve found doing it in this order prevents you from forgetting to optimize basic ultrasound settings that can drastically improve your image quality.
Adjusting the Time Gain Compensation (TGC) allows you to adjust the gain at almost any depth of your ultrasound image, not just the near and far-fields. The top rows of the Time Gain Compensation control the nearfield gain and the bottom rows control the far-field gain.
The steps to performing continuous wave Doppler are the similar to Pulse wave Doppler except where you put the sample gate does not matter. It will measure velocities across the entire cursor line.
(Editor’s note: Regarding this section, we are referring to Gain in the setting of B-mode/greyscale. You can also change the gain in your Doppler modes which we will discuss in the following section on “Advanced Modes.” Lastly, some machines have an “Autogain” button that I rarely use because I find it typically undergains your image.)
So the most important thing you can do to improve your technique for any Doppler mode is to make sure that the movement/speed of whatever you are measuring is parallel to your ultrasound probe as much as possible (zero degrees). Anything above 25-30 degrees will significantly underestimate your measurements. And if you are perpendicular, the cosine of 90 degrees = 0 and the ultrasound Doppler will read no flow or movement.
I hope you found this post helpful! Here is a Video summarizing the most commonly used ultrasound knobs, probes, and modes:
Calipers are an important feature of ultrasound machines that allows you to measure the distance of specific structures of interest.
[…] Further reading: 1. Enriquez JL and Wu TS. An introduction to ultrasound equipment and knobology. Crit Care Clin. 2014 Jan;30(1):25-45, v. doi: 10.1016/j.ccc.2013.08.006. 2. Wiafe YA and Badu-Peprah. The Influence of Ultrasound Equipment Knobology in Abdominal Sonography. In: Essentials of Abdominal Ultrasound, Gamie SAA and Foda EM (ed.) [online] 2019. DOI: 10.5772/intechopen.83713 3. Dinh V. Ultrasound Machine Basics-Knobology, Probes, and Modes. Pocus 101 [online] https://www.pocus101.com/ultrasound-machine-basics-knobology-probes-and-modes/#B-Mode_Brightness_Mod… […]
However, there are now handheld devices that connect to your smartphone and can simulate multiple probe types with just a click of the button. The Butterfly Ultrasound Device is an example of this (see below). From my experience, the footprint is slightly larger than the phased array and the weight of the probe is about 2-3 times more than a typical phased array. This increased weight is accounted for by the processor and the battery.
Continuous Wave Doppler is very similar to pulse wave Doppler except it does not alias and can detect very high velocities (greater than 1000cm/second). So Continuous Wave Doppler is the optimal choice for measuring high-velocity applications such as valvular stenosis and regurgitation.
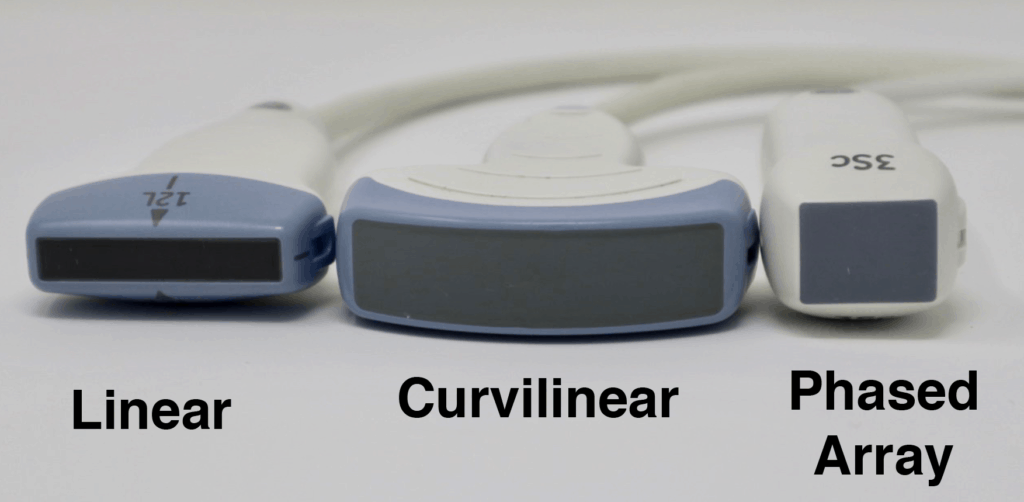
The Ultrasound Probe “Footprint” refers to the area on the probe that comes in contact with the patient’s skin in order to produce an ultrasound image. It is located at the very tip of the probe and is usually has a soft “rubbery” feel. Depending on the application you may want a smaller or larger footprint. Regarding footprint width from largest to smallest it goes: Curvilinear > Linear > Phased Array.
The curvilinear ultrasound probe has a frequency range of 2-5MHz. It is considered a low-frequency probe and has a large/wide footprint, allowing for better lateral resolution (compared to the phased array probe). The curvilinear ultrasound probe is often used for abdominal and pelvic ultrasound exams. However, it can also be used for cardiac and thoracic ultrasound exams but is limited by the large footprint and difficulty with scanning between rib spaces.
The advantage of this probe is that piezoelectric crystals are layered and packed in the center of the probe making it easier to get in-between small spaces such as the ribs (notice the extremely small pinpoint footprint on the ultrasound image below).
[…] get the Aortic Valve level from the Mitral Valve level, tilt the tail of the probe inferiorly and point it towards the Aortic […]
Ultrasound M-mode is defined as a motion versus time display of the B-mode ultrasound image along a chosen line. The motion is represented by the Y-axis and time is represented by the X-axis. Common applications for M-mode include looking at E point septal separation in cardiac scanning or calculating fetal heart rate for obstetrics. You can also use M-mode in lung ultrasound to evaluate for lung sliding and rule out pneumothorax.
Properly performing Point of Care Ultrasound involves understanding the ultrasound knobs, machine, and equipment. But you may have issues finding a resource that allows you to easily learn how to understand and use the ultrasound machine.
Each ultrasound probe will have it’s pros and cons. Usually, the most important factors to decide on are resolution, penetration, and footprint size. Here is a figure showing how penetration and resolution are affected with respect to the frequency of the transducer.
Pulse Wave (PW) Doppler allows you to measure the velocity of blood flow (at a single point). A unique aspect of Pulse Wave Doppler is that you can specify to the ultrasound machine exactly where you would like the machine to measure the velocity using the Sample Gate. It’s usually seen by two horizontal lines along your cursor. you can move your cursor and your sample gate and place it exactly where you want to measure your blood velocity.
Radiographically, the body is divided into three distinct planes: Sagittal, Coronal, and Transverse. Any combination of those movements is considered “Oblique.”
The last ultrasound setting you can use to optimize your image is by adjusting the focus. When you adjust your focus you are simply concentrating your ultrasound waves at a specific depth of the image to maximize the resolution at that depth.
These views can be obtained by rotating 90 degrees relative to each other. These terms are helpful in structures such as vascular and cardiac applications. Also, this is useful when deciding to perform a procedure in a short versus long-axis approach.
The single most important factor that will determine if you can get proper ultrasound images is choosing the correct ultrasound probe or transducer. Like with anything else you do, the right tool will be needed for the right situations. For example, if you used a linear probe, that has great resolution but minimal depth, you will not be able to visualize much if any of the heart.
Handling the ultrasound probe and proper movement is essential to obtaining optimal ultrasound images. There are traditionally 4 basic movements that are performed when scanning with ultrasound they are Slide, Rock, Tilt(Fan), Rotate. Another technique that could be considered a “5th” cardinal movement is Compression.
Conversely, if you decrease the depth you will be visualizing more superficial structures. Here is an example below of decreasing depth:
The images below demonstrate the relative sizes and footprints of the 3 most commonly used ultrasound probes (Linear, Curvilinear, and Phased Array):
Rocking the ultrasound probe involves “rocking” the ultrasound probe either towards or away from the probe indicator along the long-axis.
However, if a machine does allow you to adjust the focus, it is very important to place the focus cursor to the depth of the area of interest. Usually, the focus is indicated by a small arrow (or hourglass) superimposed on the depth markings.
POCUS 101 Tip: For learners, really trying to improve, I always suggest that when you see a suboptimal image, think to yourself what is the next best transducer manipulation you can perform to get an optimal image. Too often, learners try a random combination of transducer movements without thinking first what the image should look like prior to manipulating the transducer.
This power symbol applies to almost all ultrasound devices as well. Just look for it when you want to turn on your machine.
Unlike Pulse Wave Doppler which has a sampling gate to measure a single point along your cursor, Continuous Wave Doppler measures all points along your cursor. Therefore what you will see will be the maximum velocity of flow detected along the cursor line. This is a pro and a con. It is a pro because you don’t have aliasing and can detect high velocities, but it is a con because you don’t know exactly where that velocity is coming from on the cursor. Also if there are two velocities along the cursor line, you won’t be able to differentiate the lower velocity compared to the higher velocity signal, since the high-velocity signal will mask the low-velocity one.
The most common Doppler mode you will use is color Doppler. This mode allows you to see the movement of blood in arteries and veins with blue and red patterns on the ultrasound screen.
Selecting the correct application preset is similar in that it will automatically select the ideal frequency, depth, and gain for that application (i.e. cardiac vs abdominal). This gives you a great starting point to further fine-tune your image with the other knobs/buttons (depth, gain, focus, TGC, etc). In addition, the ultrasound will always start in B-mode or “greyscale” mode by default.
In general, for almost all standard applications and procedures the indicator orientation marker position will be on the LEFT side of the screen. In cardiac mode, the indicator orientation marker will be on the RIGHT side of the screen.
Here is what the Curvilinear probe looks like and how an ultrasound image will appear on the screen. Notice the curved nature of the ultrasound image.
[…] Para obtener cada punto de referencia en las vistas discutidas a continuación, la sonda de ultrasonido a menudo necesitan ser manipulados en un número de orientaciones. […]
I would suggest that if you are just starting out, focus on B-mode (greyscale), and get really good at obtaining high-quality 2D images. After you feel comfortable with B-mode start adding on and learning the other more advanced Doppler modes. You can always come back to this post as a reference when you are ready to use the other modes!
Below we are rotating between a short-axis and long-axis of the brachial artery using a clockwise rotation of 90 degrees.
The endocavitary probe has a curvilinear footprint with a wide view but has a much higher frequency (8-13 MHz) than a curvilinear ultrasound probe. The image resolution of the endocavitary probe is exceptional, but like the linear probe, it must be adjacent to the structure of interest since it has such a high frequency/resolution, but poor penetration.
Accessing the Tissue Doppler function will vary by machine but usually just involves pushing a knob/button labeled “TDI” (Tissue Doppler Imaging) while you are in the Pulse Wave Doppler mode.
Besides B-mode and M-mode you will have other advanced ultrasound Modes that involve “Doppler.” Here is an image of all the available ultrasound modes:
The “probe indicator” on the ultrasound probe can be identified as an orientation marker (ridge, indentation, groove, or nub) on one side of the probe. This corresponds to the indicator or orientation marker on the ultrasound image.
Most ultrasound machines will have settings that allow you to fine-tune and adjust the gain at specific depths of your greyscale ultrasound image. These will be termed Near/Far field gain or Time Gain Compensation (TGC).
B-mode is the single most important mode you need to master in order to be proficient at point of care ultrasound (POCUS). All of the other modes rely on you getting a good B-mode (2D) image. Fortunately, we already discussed the most common ultrasound settings for B-mode in the ultrasound Knobology section above.
(Editor’s note: for the Butterfly. You don’t actually have to switch between transducers because it is an “all-in-one” device. When you switch the application preset it will automatically simulate the correct transducer settings for you)
The right side of the screen will have dots or lines that correspond to the depth in centimeters. This can give you an estimation of how deep your structures are as well. As you INCREASE the depth setting on your machine, you will see the numbers increase on the right side of the screen to correspond to the depth of penetration.
Here is an example of the long axis and short axis of the heart. The parasternal short axis is obtained by rotating 90 degrees clockwise from the parasternal long axis view.
There is a mode similar to color Doppler that you may encounter called Power Doppler. This mode does not show up as red or blue on the screen but only uses a single yellow color signifying the amplitude of flow. So you can’t tell if the flow is going towards or away from the probe given that it has only one color. It is more sensitive than color Doppler and is used to detect low flow states such as venous flow in the thyroid or testicles.
In the example below, we are going from a short axis to the long axis of the brachial artery by rotating clockwise 90 degrees:
Tilting the ultrasound probe involves moving the transducer from side to side along the short axis of the probe. It is commonly also called “Fanning” as well. Tilting will allow visualization of multiple cross-sectional images of a structure of interest. You can apply this technique to structures such as the heart, kidney, bladder, vessels, etc.
Just like the world implies, the “freeze” button freezes a frame for you so you have time to view it in more detail. The ultrasound machine will usually store a 10-30 seconds of data and you can scroll back to see previous frames as well.
Compression with the ultrasound probe involves putting downward pressure on the probe to evaluate the compressibility of a structure or organ of interest. The most common use is to evaluate for deep vein thrombosis, differentiate between artery versus vein, and evaluation for appendicitis (non-compressible).
All ultrasound machines will allow you to save an image and/or video clip of your ultrasound scan. This is important if you are trying to archive, bill, or use any ultrasound images/videos as teaching files.
Each transducer will have a different list of application presets based on its frequency and footprint. The ultrasound device companies will create application presets that make sense for those specific probes.
This is an interesting fact: the on and off buttons were derived from a binary numbering system where “0” was for OFF and “1” was for ON. So to create the universal symbol for Power the “0” and “1” were combined to make the following symbol:
A common question that comes up with color Doppler is: What do the colors on ultrasound mean? The answer is: RED means there is flow TOWARDS the ultrasound probe and BLUE means that there is flow AWAY from the ultrasound probe. It is a misconception that red is arterial and blue is venous. It actually just depends on the direction blood is flowing relative to the angle of your ultrasound beam.
Here is an example of decreasing the TGC of the middle of the image with a corresponding absence of echoes on the middle of the ultrasound screen.
This is why you can’t use this mode for very high-velocity applications such as severe regurgitation or stenosis of the heart valves. Here is an example of aliasing with pulse wave Doppler:
The good news is that all of the principles of Pulse Wave Doppler also apply to Tissue Doppler. In fact, Tissue Doppler is just another form of Pulse Wave Doppler that allows you to measure the much slower speeds of tissue/muscle movement (from 1cm/s – 20cm/s) compared to Pulse Wave Doppler that measures the much faster speed of blood (30cm/s – 200cm/s).
The commonly used Sonosite M-Turbo or Edge machines allow you to adjust the “Near field” and “Far field” gain of your ultrasound images. The near field refers to the top half of the ultrasound screen and the far field refers to the bottom half of the ultrasound screen. The overall gain is just called “Gain” and is on the bottom left-hand corner of the Sonosite machine buttons.
The first of these ultrasound settings you should adjust is the depth. The ultrasound depth setting is simply how deep you want the ultrasound machine to be able to scan.
Initially, these Doppler modes may seem confusing but in reality, all Doppler settings are simply meant to detect speed going either Towards or Away from your probe (check out our previous post on Doppler Physics HERE). Understanding this is the first step to mastering ultrasound Doppler.
Sliding involves moving the entire probe in a specific direction to find a better imaging window. This is usually used to find the best window, move to different areas of the body, or to follow a specific structure (such as a vessel).
Think of selecting the ultrasound application preset like how you would select the correct preset for your point and shoot camera. You would use a different setting for day mode versus light mode. The camera will help adjust the settings to optimize for those specific conditions.
If you went through the previous steps then you should have a really good and optimized image. Here are just some other buttons you may encounter that may be useful if you need to freeze, measure, or capture your ultrasound image.
POCUS 101 Tip: Sometimes, you may be in a different mode or ultrasound machine setting and may wonder how to just reset your settings. Usually pushing the B-mode or 2D button on the ultrasound machine will reset everything and bring you back to the simple B-mode setting.
The rule of thumb is to only use as much depth that is necessary to see your structure of interest. Often times for beginning users, their depth will be too high and there is a lot of wasted “Ultrasound Real Estate” on the bottom of the screen.
This seems like common sense but I’ve seen many learners just want to jump in and start scanning with the wrong transducer. Unfortunately, understanding all of the ultrasound knobs won’t mean much if you have the wrong ultrasound probe to start off with!
Below is a quick video demonstrating how to use all of these functions (freeze, measure, image capture) by measuring the LVOT (left ventricular outflow tract) diameter. You can use this same technique to measure any other structure of interest.
Ultrasound gain simply means how bright or dark you want your image to appear. It increases or decreases the strength of the returning ultrasound signals that you visualize on the screen.
If you read the beginning of this post, you should already know what ultrasound probe you need to use based on the application you are performing. So after turning on the ultrasound machine, the next most important step is to switch to the correct ultrasound transducer you will need.
Below is an example of how the M-mode (left side of screen) and B-mode (right side of screen) compare when looking at lung sliding. M-mode simply takes a “slice” of your B-mode image where the cursor line is placed and translates that “slice” over time. It ignores everything else on the B-mode scan except for where you have that cursor line. You can see on the Y-axis how the structures (subcutaneous tissue, muscle, and pleural line) correlate between the M-mode and B-mode images. You can also see the relative motion of these structures over time (X-axis).
All ultrasound machines will have an “Overall” Gain setting that, when increased or decreased, will make the entire ultrasound image brighter or darker. This is good to use when your entire imaged is too dark (under-gained) or too bright (over-gained).
Now the application preset will usually give you a decent image right when you place the ultrasound probe on the patient. However, there are some ultrasound settings that may need to be adjusted to optimize your ultrasound settings further.
All Doppler signals (regardless of which Doppler mode you are using) are calculated using the Doppler Shift Equation. Below is a figure detailing how the Doppler Shift is used and how the angle of insonation is extremely important in what the transducer will detect as the speed of flow/movement. For any type of Doppler, you want the flow/movement to be going directly towards your probe (zero degrees). As you move more towards a 90-degree angle there will be no flow detected by the ultrasound machine.
It is very important that you master each of these ultrasound transducer manipulation/movement techniques. Most experienced sonographers think what manipulation or combination of movements will give them the desired image. In their minds, they know how each transducer manipulation should change their image. With deliberate practice, you will be able to do this too!
(Editors Note: There is some more recent literature that suggests that the term “sliding” should indicate motion along the long axis of the probe and “sweeping” involves motion along the short axis of the probe. However, I have found this confuses learners more than just the general term sliding to encompass any movement of the probe from the original position. Also sometimes when you are sliding you are not just going along the short or long axis of the probe but a combination. However, I wanted to mention this distinction in case you encounter it)
After switching to the correct ultrasound probe, the next step is to select the correct application preset for that transducer.
Now it may seem daunting when thinking about all of the available ultrasound modes available. In this section, the most common and basic ultrasound modes: B-mode and M-mode. In the following section, I will cover the more advanced Doppler Modes.
(Editor’s note: I’m using the velocity of blood as the example here. But the same principles apply if you are measuring muscle movement using tissue doppler.
This post mainly goes over ultrasound machine settings, probes, buttons, and functions. I also created another post on a simple way of learning Ultrasound Physics and Artifacts you can access by clicking HERE.
The phased array (or sector array) transducer is commonly branded as the “cardiac probe” and has a frequency range from 1-5MHz. It has a similar frequency range as the curvilinear probe but has a smaller and flat footprint.
In this post we will go over the 4 most common Point of Care Ultrasound probes you will encounter (linear, curvilinear, phased array, and endocavitary probes). The table below lists when you should think about using each type of ultrasound probe.
This is really great ,it has cleared my basic concepts and lessen the confusion of handling the machine which nobody teaches this way. Kindly guide how can I connect with you for further guidance regarding ECHO. Kind Regards.
When you are in one of these Doppler settings, you will be able to optimize your image further by adjusting the following ultrasound buttons/knobs:
The biggest limitation with Pulse Wave Doppler, however, is that there is a limit on the maximum speed you can detect. Anything past this limit (termed Nyquist Limit) will cause the signal to alias. In general, you do not want to use Pulse Wave Doppler for any applications that require measuring speed above 200cm/second.
Most other ultrasound machines will allow you to further adjust the gain in even more specific areas of your ultrasound screen. This ultrasound setting is called “Time Gain Compensation” or TGC.
Here is an example of measuring tricuspid regurgitation (TR) using continuous wave Doppler. Notice how CW Doppler can measure the high velocity of this TR jet (344cm/s).
It is the ideal probe for cardiac scanning however it can perform all of the applications the curvilinear probe can as well (with less lateral resolution).
Rotating the ultrasound probe involves turning the transducer in a clockwise or counterclockwise direction along its central axis. Rotation is most commonly used to switch between the long and short axis of a specific structure such as a vessel, the heart, the kidney, etc.
In this post, I will go over the most common Ultrasound Knobology (knobs/buttons), Probes, Modes, Movements, Orientations, and Planes you will need to properly scan. By learning these ultrasound basics, you will be able to have the fundamentals on how to use any ultrasound machine you may encounter!
Now some learners may feel like the “other doppler modes” such as Pulse wave, Continuous wave, and Tissue Doppler are very advanced settings. However, the same principles of color Doppler apply to these other Doppler modes as well. The ultrasound probe is just detecting flow or motion either TOWARDS or AWAY from it. If flow/motion is towards the probe there will be a positive deflection and if it is away from the probe there will be a negative deflection.
The linear ultrasound probe is a high-frequency transducer (5-15 MHz) that will give you the best resolution out of all of the probes but is only able to see superficial structures. A general rule of thumb is that if you are going to ultrasound anything less than about 8cm, then use the linear probe. Anything above 8cm you won’t be able to see much.
Rocking allows you to help center the area of interest. This is also referred to as “in-plane” motion because the image is kept in-plane throughout the manipulation.



 Neil
Neil 
 Neil
Neil