
KHS-12 3 Wire Surveillance Kit - Kenwood NX-5200 Portable ... - 5200 12
An interesting finding of this observational study was the absence of relevant complications, including endophthalmitis, RPE tears, retinal breaks or detachment and IOI, vasculitis, or vascular occlusion in the treated patients, unlike in the phase III HAWK and HARRIER studies, where an overall rate of 4.6% of any IOI was reported.27 This result may be due to the limited sample, the differences in patient characteristics, and the pathology treated. As reported by the American Society of Retina Specialists, most IOI events occur in females, although females constituted less than 40% of our sample. Additionally, the anatomic characteristics of PNV associated with chronic CSC may differ from that of wet age-related macular degeneration, which could potentially influence the rate of IOI. Larger studies are needed to further investigate this issue.
The family owned appeal of this company is gone. Upper management is ready for retirement and lacks real direction, Recent high rate of turnover in key ...
Central foveal thickness decreased from 317.8 ± 109.3 µm to 254.5 ± 72.9 µm at 1 month after the first injection (P = 0.007) and to 239.8 ± 74.8 µm at the end of the follow-up period (P = 0.0005). Similarly, SCT decreased from 399.3 ± 86.2 µm to 362.5 ± 96.4 µm at 1 month after the first injection (P = 0.002) and to 355.5 ± 92.7 µm at the end of the follow-up period (P = 0.0008).
Before starting brolucizumab, 23 eyes showed subretinal fluid, 8 both subretinal and intraretinal fluid, and 3 intraretinal fluid only. At the last visit, 22 eyes (64.7%) showed complete reabsorption of both intraretinal and subretinal fluid, whereas subretinal fluid was still present in 8 eyes (23.5%), and both intraretinal and subretinal fluid in 4 eyes (11.8%). The mean number of brolucizumab injections required to achieve complete fluid reabsorption was 2.8 ± 1.8. central foveal thickness decreased from 317.8 ± 109.3 µm to 239.8 ± 74.8 µm (P = 0.0005) and subfoveal choroidal thickness decreased from 399.3 ± 86.2 µm to 355.5 ± 92.7 µm at the end of the follow-up period (P = 0.0008). The mean logarithm of the minimum angle of resolution best-corrected visual acuity improved from 0.4 ± 0.2 to 0.3 ± 0.2 at 1 month after the first injection and remained stable at the same values at the end of the follow-up period (P = 0.04).
Correspondence: Roberto dell'Omo, Department of Medicine and Health Sciences “Vincenzo Tiberio”, University of Molise, Via Francesco De Sanctis 1, Campobasso 86100, Italy. e-mail: roberto.dellomo@unimol.it
Safe, smart and scalable, ProCuity Bed Series is a versatile, low-height bed for all patient care environments – from MedSurg units to the ICU. Featuring wireless connectivity with advanced fall prevention technologies, it is designed to enhance patient and caregiver safety.
StrykerZoombed
“Partial response” and “no response” to previous anti-VEGF treatment were defined as follows: resolution of intraretinal fluid and reduction of subretinal fluid thickness of 10% or more in comparison with baseline was considered as “partial response”; persistent intraretinal fluid and/or reduction of subretinal fluid thickness of 10% or less in comparison with baseline was considered as “no response.”
Central serous chorioretinopathy (CSC) is a disease that falls under the pachychoroid spectrum,1 characterized by choroidal thickening and hyperpermeability, along with a serous detachment of the neurosensory retina and/or the retinal pigment epithelium (RPE). Although most CSC cases resolve spontaneously within 3 months from onset, approximately 10% of patients may experience multiple recurrences or progress to a chronic course. Chronic CSC is characterized by multifocal, irregularly distributed RPE changes associated with photoreceptor damage and persistence of subretinal fluid that can predispose patients to develop pachychoroid neovasculopathy (PNV). After an average of 17 years of disease duration, the prevalence of PNV has been reported to be as high as 24%.2
Brolucizumab (Beovu, Novartis Pharma AG) is a recently developed anti-VEGF agent that consists of a humanized single-chain antibody fragment with a molecular weight of 26 kDa, characterized by a more sustained duration of action than other anti-VEGF agents.11 The smaller molecular size and the lack of Fc domain12 provide for potentially more effective penetration of the retina and choroid than other anti-VEGF molecules. Because of these characteristics and the high affinity to all VEGFA isoforms, brolucizumab may have a more potent effect on choroidal vasculature and PNV when compared with other anti-VEGF therapies.
StrykerHospital beds price
Intuitive Patient and Bed Monitoring Systems: ProCuity's exclusive Adaptive Bed Alarm uses load cell technology to sense a patient's weight and alert nurses if a patient is out of position or has left the bed. With ProCuity's iBed™ Watch system, all operational aspects of the bed, including side rail positioning, head of bed angle and height, are monitored. Caregivers are alerted if any components are out of position.
Eyes that had previously received photodynamic therapy (PDT) and/or mineralocorticoid antagonist agents and/or anti-VEGF, as well as eyes that had not received any prior treatment, were eligible for the study. Patients previously treated with anti-VEGF injections were eligible to be enrolled in the study only if they had received at least six injections administered on a monthly regimen (independent of the anti-VEGF drug used) with the aim of obtaining complete reabsorption of subretinal or intraretinal fluid.
Completely Wireless: ProCuity's Secure® Connect™ wireless solution allows the bed to connect without cables to nurse call systems. Additionally, with iBed Wireless, bed data, including bed configuration and exit alarm activity, are wirelessly compatible with facilities' hospital information systems (HIS)1. To help give caregivers increased visibility to safe bed configuration and bed exit alarm activity, ProCuity can also integrate with Stryker's optional patient-centric clinical dashboard, iBed Vision.
StrykerSV2
Secure .gov websites use HTTPS A lock ( Lock Locked padlock icon ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites.
On the basis of the results of the previous studies, we collected data from 34 eyes, 25 of which had received a minimum of 9 anti-VEGF injections before being switched to brolucizumab. Notably, 80% of these eyes had received six injections of the same anti-VEGF drug on a monthly basis and none had shown complete subretinal or intraretinal fluid reabsorption after the treatment. Conversely, after a mean of 3.3 ± 1.5 injections, 60% of the previously treated eyes showed complete intraretinal and subretinal fluid reabsorption. A decrease in both central foveal thickness and SCT accompanied the reabsorption of fluid. Specifically, a reduction in SCT was observed in 19 eyes, and it was more than 35 µm in 12 eyes. Because circadian changes in SCT have been reported to be less than 35 µm,14,15 and all OCT images in our sample were taken during morning working hours, we can exclude that the observed reduction was caused by physiological circadian variations of choroidal thickness rather than the effect of brolucizumab.
In this study, improvement in visual acuity was approximately one line logMAR, consistent with previous reports.8–10 Visual acuity improved or remained stable in 20 eyes and worsened in 6 eyes presumably owing to chronic RPE and retinal changes, scarring associated with neovascularization, and the age of our sample.
This study aimed to assess the anatomical and functional response of chronic CSC complicated by PNV when treated with intravitreal brolucizumab, an off-label use of this therapy.
Exclusion criteria were as follows: PDT within 6 months or intravitreal injection of anti-VEGF agents within 2 months from the first injection of brolucizumab, age-related macular degeneration, pathological myopia, retinal vein occlusion, diabetic retinopathy, hereditary retinal diseases, diseases of the vitreoretinal interface, intraocular surgery within 3 months, and any optic media that impeded sufficient image quality.
PNV was classified into three types: type 1 (neovascularization between the Bruch membrane and the RPE), mixed type 1 and type 2 (neovascularization in the sub-RPE and subretinal compartments), and polypoidal vasculopathy.13 No case of pure type 2 neovascularization was observed in this series.
Among the eight patients who had prior PDT and were subsequently treated with anti-VEGF drugs, seven showed complete reabsorption of subretinal/intraretinal fluid after switching to brolucizumab. Of these seven patients, one had been treated with ranibizumab, aflibercept, and bevacizumab (13 intravitreal injections in total) and six had received monotherapy with ranibizumab (2 patients), aflibercept (3 patients), and bevacizumab (1 patient), respectively, with a mean of 9.5 ± 0.5, 9.7 ± 0.4, and 13 injections performed, respectively.
The preliminary results of our study show that brolucizumab may induce fluid reabsorption, even in eyes that are poorly responsive to aflibercept, which is likely due to the specific physical properties of this new anti-VEGF agent. Brolucizumab inhibits all isoforms of VEGF-A17 and, with a molecular weight of 26 kDa, is the smallest clinically available anti-VEGF agent (bevacizumab, 147 kDa; aflibercept, 115 kDa; ranibizumab, 48 kDa).17,18 The smaller size of brolucizumab and the lack of the Fc domain allow for a high concentration of the drug to be delivered per intravitreal injection17,18 (Tietz J et al. IOVS 2015; 56: ARVO E-Abstract 1501) and this high concentration is supposed to allow for a high degree of RPE penetration.17,19
StrykerProCuitybedprice
Imaging was obtained at each participating centre with the same equipment, that is, a confocal scanning laser ophthalmoscope (SPECTRALIS HRA + OCT, Heidelberg Engineering, Heidelberg, Germany, version 1.9.13). The diagnosis of chronic CSC and PNV was made using fluorescein angiography, ICGA, OCT, and/or OCT angiography (if available). To differentiate between neovascularization secondary to age-related macular degeneration and PNV, the eyes enrolled in this study must fulfill the following criteria: documented history of CSC, absence of degenerative changes like geographic atrophy suggestive of AMD, absence of drusen of more than 125 µm, evidence of choroidal thickening and dilated choroidal vessels seen with OCT, and choroidal hyperpermeability seen with ICGA in areas devoid of neovascularization.
BCVA improved in 16 eyes (47%), remained stable in 10 eyes (29.5%), and worsened in 8 eyes (23,5%). Overall, the mean logMAR BCVA improved from 20/50 to 20/40 (logMAR 0.4 ± 0.2 to 0.3 ± 0.2) at 1 month after the first injection and remained stable at the same values at the end of the follow-up period (P = 0.04). The mean visual acuity at baseline was 20/63 (logMAR 0.53 ± 0.18) and slightly improved to 20/56 (logMAR 0.46 ± 0.22) in the eyes with persistent fluid at the end of follow-up (n = 12; P = 0.6). However, in the eyes with complete fluid reabsorption at the end of the follow-up period (n = 22), BCVA significantly improved from 20/61 (logMAR 0.49 ± 0.27) to 20/38 (logMAR 0.39 ± 0.29; P = 0.01).
Multimodal imaging of an eye with type 1 neovascularization complicating chronic CSC treated with intravitreal brolucizumab. At baseline, areas of patchy increased fluorescence with staining and leakage are visible in the early and late phases, along with signs of gravitational retinopathy on fluorescein angiography (A, B). ICGA shows hypercyanescent dots in the context of hypercyanescent plaques (C, D), while spectral-domain OCT (SD-OCT) shows a shallow, irregular RPE detachment associated with intraretinal fluid (E). One month after a single injection of brolucizumab, complete resolution of the intraretinal fluid is observed on SD-OCT (F). The bright green arrows on infrared pictures in (E) and (F) show the location and direction of OCT scans.
The study involved 34 patients (22 males, 12 females) with a total of 34 eyes (19 right eyes [55.9%]). At baseline (the time of the first brolucizumb injection), the mean age of the patients was 55.1 ± 9.4 years. On the basis of ophthalmoscopic examination, all patients showed macular pigmentary changes consistent with chronic CSC and five out of 34 (20.6%) patients showed drusen of less than 125 µm at the macula. Specifically, three out of five patients had drusen of less than 63 µm and two had drusen between 63 and 125 µm. The patients with drusen of less than 63 µm were ages 48, 50, and 53 years, whereas the 2 patients with drusen between 63 and 125 µm were aged 56 and 63 years.
This study has several limitations, including its observational, retrospective design, in a relatively small cohort of patients who were previously treated with different anti-VEGF drugs. However, all the patients included in this study had received at least 6 monthly injections of an anti-VEGF agent before being switched to brolucizumab. Other relevant limitations are the lack of a control group and the mixture of heterogenous eyes (naïve + non-naïve), this potentially introducing uncertainties and confounding effects. A further limitation is that the follow-up period after switching to brolucizumab was relatively short, limiting definitive conclusions about the potential longer durability of brolucizumab in comparison with other anti-VEGF therapies. VA was evaluated using a nonstandardized method (Snellen charts) and then converted to logMAR, thus reducing the reliability of the visual acuity outcome. The age of our sample and the presence of drusen in five eyes may pose the issue of neovascularization secondary to AMD instead of CSC. However, drusen were detected in only five patients and were 125 µm or smaller in all cases; in addition all patients had a history of chronic CSC, showed choroidal thickness of more than 300 µm, dilated choroidal vessels on OCT, and choroidal hyperpermeability on ICGA in areas devoid of neovascularization. Thus, AMD as a cause of macular neovascularization seems unlikely in this series. In conclusion, this study suggests that brolucizumab may be an effective option in treating PNV secondary to chronic CSC, both in naïve eyes and in eyes poorly responding to other anti-VEGF drugs. Given the rarity of this disease, it is unlikely that any prospective clinical trial will soon take place to compare brolucizumab to other anti-VEGF treatment options.
Strykersmartbed
Set at a low height of 29.2 cm, ProCuity is ergonomically designed with the latest technologies to promote safe patient handling and help reduce fall-related injuries, including intuitive patient positioning and bed alarms as well as ergonomic side rails. Helping to address nurse call cable connectivity issues prevalent in hospitals today, ProCuity can be equipped with fully wireless features. Additionally, the bed's easy-to-use touchscreens and other key components are designed to make the job of caregivers easier and more efficient, while providing for a more enhanced patient experience.
Currently, there is no standard treatment algorithm for PNV in chronic CSC. Some experts have proposed that eyes with PNV may benefit from an extended loading phase of anti-VEGF drugs compared with the standard three injections for AMD. The rationale behind this proposal is that repeated anti-VEGF injections may have a long-term effect on choroidal thickening and congestion. However, the optimal dosing regimen for these eyes remains unclear and further studies are needed to establish the best approach.
In line with previous studies8–10,25,26 (range, 57–65 years), the mean age of our sample was 55 years. This is not surprising because CSC is commonly seen in young patients but the occurrence of PNV is typically associated to chronic stages. However, only 5 patients showed drusen at the macula and in all cases the drusen were less than 125 µm. Thus, an overlap with wet age-related macular degeneration as cause of macular neovascularization seems unlikely for this series.
Considering the all group (n = 34), before starting brolucizumab, 23 eyes showed subretinal fluid on OCT, eight eyes had both subretinal and intraretinal fluid, and three had intraretinal fluid only. Regarding PNV, 18 (52.9%) were classified as type 1, 11 (32.4%) as mixed type 1 and type 2, and 5 (14.7%) as polypoidal vasculopathy.13
At the last visit (1.8 ± 0.6 months after the last brolucizumab injection), 22 eyes (64.7%) showed absence of either intraretinal or subretinal fluid, and subretinal fluid was found in eight eyes (23.5%), and both intraretinal and subretinal fluid in four eyes (11.7%). Specifically, the absence of either intraretinal or subretinal fluid was found in 7 of 9 (naïve eyes 77.8%) and in 15 of 25 (60%) of the eyes previously treated with anti-VEGF agents (P = 0.34). The mean number of brolucizumab injections required to achieve complete fluid reabsorption was 2.8 ± 1.8, specifically, 1.6 ± 0.7 for naïve eyes and 3.3 ± 1.5. for non-naïve eyes.
CA41211BN Centerset Bathroom Sink Faucets · Details add to project · alt here ... Cleveland Faucet Group, a Moen Incorporated brand, offers an unparalleled ...
Global Launch: ProCuity will be launched globally in over 70 countries, with a market focus in North America, Latin America, Europe, the Middle East, Australia/New Zealand, and Asia.
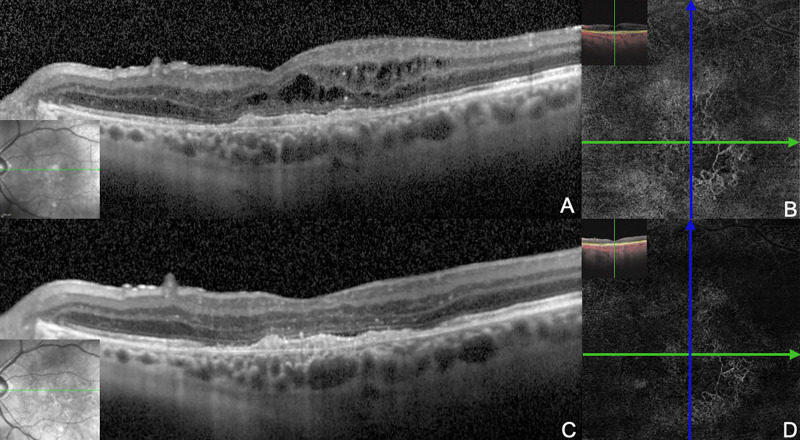
Multimodal imaging of an eye with PNV complicating chronic CSC treated with intravitreal brolucizumab. (A) At baseline, spectral-domain OCT shows a neovascular complex underneath the RPE (type 1) at the fovea associated with intraretinal fluid. (B) the OCT angiography (slab at the level of the choriocapillaris) shows the neovascular network. After three injections of brolucizumab, the intraretinal fluid has completely reabsorbed (C) and the neovascular network has shrunk (D). The green line on infrared pictures in (A) and (C) shows the location and direction of OCT scans.
KALAMAZOO, Michigan, USA, Feb. 4, 2021 /PRNewswire/ -- Stryker, one of the world's leading medical technology companies, announced its EMEA launch of a completely wireless hospital bed, ProCuity™. This bed series was designed to help reduce in-hospital patient falls at all acuity levels and improve nurse workflow efficiencies and safety. It can connect seamlessly to nurse call systems without the use of cables or wires.
The study was a retrospective case series of patients who attended seven different tertiary referral centers: the University of Molise in Campobasso, Italy; the University Magna Graecia in Catanzaro, Italy; the Santa Croce and Carle Hospital in Cuneo, Italy; "Vincenzo Monaldi" Hospital in Naples, Italy; the University of Palermo, Palermo, Italy; the University of Salerno, Baronissi, Italy; and Ludwigshafen Hospital in Ludwigshafen am Rhein, Germany. These patients were offered an off-label treatment with brolucizumab for chronic CSC complicated by PNV either because of a poor response to other anti-VEGF agents or, in naïve cases, as recommended by the surgeon after obtaining approval by the local ethics committee of each participating center. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments. Informed consent was obtained from all participants.
Official websites use .gov A .gov website belongs to an official government organization in the United States.
Among the patients treated solely with intravitreal injections before brolucizumab (N = 17), 13 received a single anti-VEGF drug; specifically, 3 patients received ranibizumab and 10 received aflibercept. Among those receiving ranibizumab, two showed a partial and one a complete response after brolucizumab, whereas of those receiving aflibercept, seven showed a partial and three a complete response after brolucizumab. Previous mean injections of ranibizumab were 10.5 in the two eyes with partial and 11 in the eye with complete response while previous mean injections of aflibercept were 11.9 ± 1.6 and 11.3 ± 1.2 in the eyes with a partial and complete response, respectively. Only 1 patient had prior treatment with eplerenone, followed by 14 injections of bevacizumab; this patient showed complete response after switch to brolucuzumab.
... 949 .577 .00 -.25 1.440 1.095 .002730 .278 .001487 .000159 1.072 .583 .00 -.25 1.520 1.092 .003174 .225 .001586 .000406 1.246 .623 .00 -.25 1.600 1.075 ...
Wall mounting provides more stability than flimsy overhead rails vulnerable to detaching. Custom Modesty Panels and Modesty Screens. Finally, if you are ...
The overall mean maximum diameter of PNV measured at baseline on ICGA images was 463 ± 186.7 µm (range, 278–649 µm) and did not differ significantly between the responder (402 ± 127.8 µm) and nonresponder group (497 ± 154.5 µm; P = 0.068).
In the MINERVA study,7 the mean number of ranibizumab injections administered for eyes affected by PNV was 5.8 over 12 months. Schworm et al.10 reported that a series of six consecutive injections of either 0.5 mg of ranibizumab or 2 mg of aflibercept effectively reduced central retinal thickness and significantly improved VA from 0.65 to 0.49 logMAR. Chhablani et al.8 reported a VA change from 0.59 to 0.48 logMAR with a mean number of 4.45 ± 4.10 injections of bevacizumab, ranibizumab, or aflibercept. In this latter study, the mean central macular thickness did not change significantly during the follow-up period compared with the baseline.
1 Nov 2017 — Shiboya as the native of the Luhya community of the western part of Kenya may call him, is attending a traditional festival in which he is sitting with all the ...
Among the eyes with complete fluid disappearance (n = 22), only five (23.8%) required five or more injections to achieve this result. Fifteen of 22 eyes (68.2%) showed complete resolution of intra/subretinal fluid after three or fewer injections, and among these, seven eyes (4 naïve and 3 non-naïve) showed complete resolution after just one injection (Figs. 123–4). The three non-naïve eyes had previously received a mean of 13.1 intravitreal injections (range, 9–25).
The BROCS study group includes Teresio Avitabile3, Vincenza Bonfiglio7, Ciro Costagliola8, Andrea D'Albenzio1, Mariaelena Filippelli1, Gianluigi Manzi5, Giorgio Randazzo2, Michele Rinaldi8, Nicola Rosa9, Vincenzo Scorcia2, Maria Vadalà7, Agostino Vaiano4, and Federico Venturi1
Standard, Customizable Platform: From MedSurg units to the ICU, the ProCuity bed series is designed to meet all patient acuity levels making standardization across hospitals easier, while reducing hospital costs associated with renting specialty beds and the need for bed transfers and extra staff.
The 20 eyes (80%) treated with a single drug (i.e.. aflibercept, ranibizumab. or bevacizumab only) received the first six injections (independently of the anti-VEGF drug used) on a monthly regimen with the aim of obtaining complete reabsorption of sub/intraretinal fluid. The other five eyes (20%) received at least three injections with the same anti-VEGF drug before switching to another. After anti-VEGF injections (other than brolucizumab), 19 eyes (76%) had shown a partial response, whereas 6 eyes (24%) had shown no response to treatment (Table). None of the eyes had shown complete sub/intraretinal fluid reabsorption. The mean number of anti-VEGF injections administered (before switching to brolucizumab) was 11.2 ± 3.4 (range, 8–13) in the group with a partial response and 13.5 ± 2.5 (range, 9–15) in the group with no response.
RES DARK FIRE E612. Breed: Angus. Registration: 18746402. Tattoo: E612. Born: 9/29/16. From: Robert Elliott & Sons, TN Canada. Eligible: Yes.
Enhanced Patient Experience: To provide greater flexibility for taller patients, ProCuity has an integrated bed extender, which allows the bed to stretch an additional 30 cm in length. It also comes with a USB port and holder to allow patients to charge and store personal electronic devices like phones.
To evaluate the anatomical and functional outcomes of intravitreal brolucizumab in eyes with chronic central serous chorioretinopathy complicated by pachychoroid neovasculopathy.
"Patient safety is at the foundation of everything we do at Stryker. With rising acuity rates leading to increased bed demand, coupled with the continuing challenge of in-hospital falls, we needed to find a solution to further enhance our response to some of today's most pressing healthcare challenges," said Jessica Mathieson, VP/GM of Acute Care, Stryker. "Leveraging our long history in innovation, ProCuity is the culmination of years of extensive research and feedback from nurses and other healthcare professionals. It was designed to improve patient outcomes and assist caregivers for years to come."
Overall, 13 eyes in this series (38.2%) still presented with some degree of sub/intraretinal fluid at the end of follow-up, with type 1 neovascularization responding better to brolucizumab than mixed type 1 and type 2 and polypoidal vasculopathy. The persistence of the fluid is likely because neovascular membranes in pachychoroid disease contain matured vessels,22 which are known to respond poorly to anti-VEGF treatment.23 In such cases, the rationale behind treatment with anti-VEGF agents is to decrease choroidal thickness and hyperpermeability, but the effect on subretinal fluid may be limited.2,24,25 Thus, despite having a higher molar dose and enhanced tissue penetration capacity, brolucizumab may have limitations in effectively treating PNV and improving VA in eyes with chronic CSC, similar to other anti-VEGF drugs. Although the sample analyzed in this series is too small to draw definite conclusions, it is noteworthy that seven of eight eyes that had been treated with PDT before receiving anti-VEGF injections showed complete reabsorption of sub/intraretinal fluid after switching to brolucizumab. Thus, PDT may play an important role, synergistic with the action of anti-VEGF agents, in promoting the complete resolution of subretinal or intraretinal fluid in eyes with chronic CSC complicated by PNV. Conversely, based on the data from this study, we failed to find an association between the final response to brolucizumab and the type of anti-VEGF agent used or the number of injections performed before switching to brolucizumab.
Keywords: brolucizumab, central serous chorioretinopathy, pachychoroid vasculopathy, vascular endothelial growth factor, optical coherence tomography
Intravitreal injections of brolucizumab were given on a monthly basis to achieve complete resolution of subretinal and/or intraretinal fluid as determined by spectral-domain OCT.
Horizontal OCT sections acquired in high-resolution or high-speed mode, covering an area of at least 20° (horizontal) × 20° (vertical) with a distance of approximately 60 to 120 µm were reviewed for analysis. The central foveal thickness, defined as the distance (µm) between the internal limiting membrane and the outer border of the RPE, was automatically measured within the central 1-mm-diameter circle of the ETDRS grid using the thickness map generated by the Heidelberg Eye Explorer software V.2 (Heidelberg Engineering, V.2.4.1, Heidelberg, Germany). Subfoveal choroidal thickness (SCT) was assessed manually by measuring the distance between the RPE and the choroidal-scleral interface under the center of the foveal depression. The presence and location of distribution of the fluid (subretinal and/or intraretinal) was qualitatively assessed. All OCT images were captured during morning hours (i.e., from 8 am to 2 pm).
StrykerProCuitybedmanual
PNV usually develops underneath the RPE, but in some cases, concomitant neovascularization above the RPE,3 or polyps, may be found.4 The subretinal fluid observed in association with PNV may be related to the PNV itself or caused by the underlying hyperpermeable pachychoroid.5,6 Intravitreal ranibizumab (Lucentis, Novartis Pharma AG, Basel, Switzerland) has been used as on-label first-line treatment for PNV associated with chronic CSC since the publication of the MINERVA study.7 However, further studies have shown that other anti-vascular endothelial growth factor (VEGF) agents, such as bevacizumab (Avastin; Genentech, South San Francisco, CA) or aflibercept (Eylea; Bayer HealthCare Pharmaceuticals, Berlin, Germany), can be equally or even more effective than ranibizumab in treating PNV complicating chronic CSC.8–10
To our knowledge, this study is the first to investigate the effects of intravitreal brolucizumab in eyes with PNV complicating chronic CSC. The study demonstrated that almost 65% of the treated eyes achieved complete sub and/or intraretinal fluid reabsorption, with 15 of 21 eyes requiring 3 or fewer injections. Notably, in seven eyes, complete fluid reabsorption was achieved after just one injection, and three of these seven eyes had received at least nine injections of other anti-VEGF agents without success. BCVA improved or remained stable in 80% of the eyes during the follow-up period.
Incomplete reabsorption of subretinal and intraretinal fluid was observed at the end of the follow-up period in 12 eyes: 4 of 18 eyes (22.2%) with type 1 NV, 5 of 11 (45.4%) with mixed type 1 and type 2 NV, and 3 of 5 (60%) with polypoidal vasculopathy.
Regarding differences naïve and non-naïve eyes, BCVA at baseline was 20/52 (logMAR 0.41 ± 0.35) in naïve and 20/56 (logMAR 0.44 ± 0.25) in non-naïve eyes, respectively (P = 0.8). One month after the first injection of brolucizumab, BCVA improved to 20/38 (logMAR 0.29 ± 0.28) in naïve and to 20/46 (logMAR 0.36 ± 0.28) in non-naïve eyes and further improved to 20/30 (logMAR 0.18 ± 0.23) in naïve and to 20/40 (logMAR 0.30 ± 0.25) in non-naïve eyes at the last follow-up.
Retrospective analysis of 34 eyes treated with intravitreal brolucizumab. Twenty-five eyes (73.5%) had been treated with other anti-vascular endothelial growth factor agents before switching to brolucizumab, whereas nine eyes were naïve. Outcome measures included the change of central foveal thickness and subfoveal choroidal thickness, evaluation of sub/intraretinal fluid on optical coherence tomography, and change in best-corrected visual acuity.
The study's main objective was to assess the effectiveness of intravitreal brolucizumab in achieving complete resolution of sub/intraretinal fluid associated with PNV in chronic CSC.
About StrykerStryker is one of the world's leading medical technology companies and, together with its customers, is driven to make healthcare better. The company offers innovative products and services in Orthopaedics, Medical and Surgical, and Neurotechnology and Spine that help improve patient and hospital outcomes. More information is available at www.stryker.com.
Intravitreal brolucizumab may represent an option in patients with pachychoroid neovasculopathy complicating chronic central serous chorioretinopathy.
Multimodal imaging of an eye with polypoidal vasculopathy complicating chronic CSC treated with intravitreal brolucizumab. At baseline, fluorescein angiography (A, B) and ICGA (C, D) show serosanguineous retinal pigment (RPE) detachments at the macula and nasally to the optic disc, along with polypoidal lesions at the infero-nasal aspect of the macula and nasally to the optic disc (white arrowheads). Spectral-domain OCT (OCT) shows RPE detachments, subretinal fluid, and intraretinal hard exudates at the macula (E). After three intravitreal brolucizumab injections, the polypoidal lesions are hardly visible on ICGA (F, G), the RPE detachments have completely flattened, and the subretinal fluid has reabsorbed on OCT (H). Note also the thinning of the choroid compared with the baseline. The green arrows in (A), (C), and (F), show the location and direction of the OCT scans shown in (E) and (H).
StrykerProCuitybedweight limit
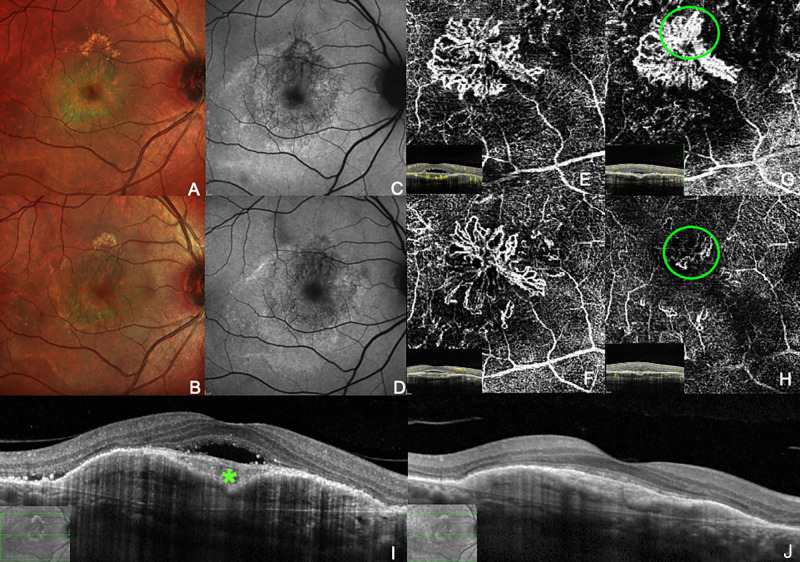
Multimodal imaging of an eye with mixed type 1 and type 2 neovascularization complicating chronic CSC before (A, C, E, G, I) and after (B, D, F, J) treatment with intravitreal brolucizumab. A, At baseline, hard exudates are visible on the false-color image around the fovea and in the upper aspect of the macula. (C) Blue-fundus autofluorescence (B-FAF) shows stippled hypo- and hyperfluorescence, sign of chronic RPE changes, in the macular area. The neovascular network underneath the RPE (E) and underneath the retina (green circle, G) are visible on OCT angiography. Structural spectral-domain OCT shows a heterogeneous reflectivity in a fibrovascular, bilobed RPE detachment along with a subretinal neovascular complex, subretinal hyperreflective exudative material (asterisk) and subretinal fluid (I). Two months after a single injection of brolucizumab, the hard exudates have reduced (B, D), the neovascularization networks underneath (F) and above the RPE (green circle, H) have decreased in size, the RPE detachment has flattened, and the subretinal fluid has disappeared (J). The green lines on infrared pictures in I and J show the location and direction of OCT scans.
For example, Chhablani et al.8 reported that eight eyes showed a poor response to intravitreal ranibizumab and intravitreal bevacizumab, but responded well to aflibercept. Jung et al.9 and Schworm et al.10 also reported the superior effect of aflibercept in comparison with ranibizumab on decreasing central retinal thickness and reabsorbing the subretinal fluid.
For all patients included in the study, at least two ICGA examinations were available: one recorded at the time of chronic CSC diagnosis and the other at the time of PNV diagnosis. The diagnosis of chronic CSC dated back to 75.2 ± 32.1 months (range, 23–120 months), whereas the diagnosis of PNV complicating chronic CSC dated back to 25.7 ± 18.6 months (range, 12–84 months). Before developing PNV, eight eyes (23.5%) had received PDT treatment and one patient had been prescribed oral eplerenone (25 mg/d for 7 days, then 50 mg/d for 2 months).
After the development of PNV, 25 eyes (73.5%) had been treated with anti-VEGF agents before receiving brolucizumab. Specifically, 13 eyes (52%) received aflibercept, 5 eyes (20%) received ranibizumab, 2 eyes (8%) received bevacizumab, 3 eyes (12%) received ranibizumab + aflibercept, and 2 eyes (8%) received bevacizumab + ranibizumab + aflibercept. Nine patients (26.5%) included in the study had not received any previous anti-VEGF treatment (naïve group) The mean number of anti-VEGF injections per patient before switching to brolucizumab was 12.4 ± 4.6 (range, 9–33), with 11 patients receiving 9 or 10 injections, 3 patients receiving 11 or 12 injections, and 11 patients receiving more than 12 injections. A summary of type and number of prior anti-VEGF treatments and relative results is provided in Table.
Stryker Corporation or affiliated entities own, use or have applied for the trademarks or service marks: iBed, ProCuity, Secure Connect, IsoTour, Stryker. All other trademarks are trademarks of their respective owners or holders. The absence of a product, feature, or service name, or logo from this list does not constitute a waiver of Stryker's trademark or other intellectual property rights concerning that name or logo.
Articles from Translational Vision Science & Technology are provided here courtesy of Association for Research in Vision and Ophthalmology
CENTAURO-ID-200-3750. $39,900. Kilo. Blanca. APLICA DESCTO ROLLO COMPLETO (sin revisar) JORDYV2BCOD-609000040351. 22 disponibles. CENTAURO-ID-200-3750 cantidad.
During the follow-up period, no cases of intraocular inflammation (IOI), vasculitis, vascular occlusion, endophthalmitis, RPE tears, and retinal breaks and/or detachment were observed in any of the treated eyes.
The Fluke Biomedical ESA612 Electrical Safety Analyzer Auxiliary leakage (hereafter the Analyzer) is a full-featured, compact, Lead isolation (Mains on applied ...
In the present study, we observed complete sub/intraretinal fluid reabsorption in nine eyes previously treated with aflibercept (aflibercept alone, 4 eyes; aflibercept + bevacizumab and/or ranibizumab, 5) without success. However, six eyes that had not responded to aflibercept injections did not respond to brolucizumab either.
Normally distributed data are presented as mean ± standard deviation in the descriptive statistics. Best-corrected visual acuity (BCVA) was measured based on Snellen charts and converted to the logarithm of the minimum angle of resolution (logMAR) for statistical analysis. Functional and structural findings were evaluated at baseline, 1 month after the first brolucizumab injection, and at the final follow-up visit. Changes after treatment were analyzed using an analysis of variance test with Bonferroni correction and Friedman test for continuous and categorical variables, respectively. P values of less than 0.05 were considered statistically significant. Statistical analysis was conducted using MedCalc version 11.5.1 (MedCalc software, Mariakerke, Belgium).
Ergonomic Side Rails: Three-position Secure® Assist side rails allow for easier patient entry and exit as well as nurse-patient interaction. By working in a "clocking motion," the side rails stay tightly close to the bed, thus avoiding interference with any real estate next to the bed.
Shop Hospital Bed Mattress Extender - Bed Extender for Bedroom and Hospital Beds - Adjustable Entrapment Prevention Safety - Prevents Zone 3 and 7 ...
Stryker bedremote Control
Chronic CSC was defined as the presence of RPE changes in the macular region; subretinal fluid in the foveal region for at least three months, with or without serous pigment epithelial detachment on optical coherence tomography (OCT); areas of leaks and/or pigment epithelial detachment on fluorescein angiography; and abnormal, dilated choroidal vasculature and choroidal vascular hyperpermeability with evidence of leaking areas on indocyanine green angiography (ICGA). Features suggestive of PNV on fluorescein angiography and ICGA included neovascular networks in the early phases with staining and leakage in the late-phase photographs. Angiographic images were independently assessed by two experienced retinal specialists (A.C. and M.F.) who judged whether or not angiographic criteria for the diagnosis of PNV were fulfilled.
– The design shown is a stencil template that is constructed of flexible semi-transparent Mylar plastic which is used for marking quilts and other crafting ...
Specifically, SCT at baseline was 383.6 ± 55.9 µm and 406.5 ± 97.3 µm in the responder and in the nonresponder group, respectively (P= 0.17). One month after injection, the SCT was decreased to 332.3 ± 80.2 µm and 376.1 ± 101.9 µm and in the responder and in the nonresponder group, respectively (P = 0.27). At the end of the follow up period SCT was 321.3 ± 64.7 µm and 366.1 ± 95.8 µm in the responder group and in the nonresponder group, respectively (P = 0.22).

In the HAWK and HARRIER studies, brolucizumab was superior to aflibercept in reducing the central subfield thickness and rates of retinal fluid at week 48, and these anatomical outcomes were maintained up to week 96.19,20 Additionally, in a study comparing the efficacy of brolucizumab versus aflibercept in Japanese participants with polypoidal choroidal vasculopathy in the HAWK trial, the fluid resolution was greater with brolucizumab at weeks 48 and 96.21
Disclosure: M. Carosielli, None; A. Carnevali, None; M. Fallico, None; E. Pirozzi, None; F. Chiosi, None; A. Chronopoulos, None; P. Cucciniello, None; M. Affatato, None; G. Rapino, None; R. dell'Omo, None
Taken together, these findings suggest that brolucizumab may be a promising treatment option for eyes with naïve and recalcitrant PNV complicating chronic CSC. Previous studies have documented the alleged superiority of aflibercept over other anti-VEGF agents in treating PNV associated with chronic CSC, attributing this superiority to the additional molecular targets and different mechanisms of uptake in the tissue of aflibercept compared with bevacizumab and ranibizumab.8–10,16



 Neil
Neil 
 Neil
Neil